Medical History Drives 76% of Diagnoses
The Power of the Patient Story

Medical History Drives 76% of Diagnoses
In an era defined by high resolution imaging and complex genetic sequencing, it is easy to assume that the most critical medical insights come from advanced machinery. However, decades of clinical research consistently reveal a different truth. The most potent diagnostic tool available to a physician is not a laboratory test or a radiological scan; it is the comprehensive narrative of the patient history.
For modern healthcare systems, particularly those in rapidly developing markets, the ability to capture and track this history longitudinally is not just an administrative task. It is the primary driver of clinical accuracy and patient safety.
The Statistical Weight of History
The diagnostic value of a patient history is one of the most replicated findings in the history of clinical medicine. A landmark prospective study of medical outpatients conducted by Peterson et al. (1992) demonstrated that medical history alone led to the correct diagnosis in 76% of cases.
In this study, physical examinations contributed just 12% to the final diagnosis, while laboratory investigations accounted for only 11%. This was not an isolated finding. It replicated the results of a 1975 British Medical Journal study by Hampton et al. which reported that history alone drove an even higher figure of 83%.
More recently, a 2022 NYU meta estimate across multiple decades of research confirmed a mean diagnostic accuracy from history alone of 75.9%. This evidence proves that the patient story is the fundamental substrate of clinical reasoning. When this story is fragmented by paper records or disconnected digital silos, the core engine of diagnosis is compromised.
From Snapshots to Sequential Context
While a single clinical encounter provides a snapshot, longitudinal health records provide the full movie. Longitudinal data extends the inherent diagnostic power of history by adding the critical dimension of time.
The OpenHIE framework emphasizes that a shared longitudinal record enables a physician to determine whether a specific clinical sign, such as elevated blood pressure or a fluctuating lab value, is a new development or a long standing baseline. This distinction is the foundation of proactive medicine.
In Sub Saharan Africa, where 89% of chronic kidney disease cases often go unrecognized until they reach a crisis stage, the ability to see a declining eGFR over several years is a life saving capability. A single "normal" result can mask a dangerous downward trend that only becomes visible when data is plotted chronologically.
The Cost of Information Gaps
Information gaps are a root cause of medical errors globally. National burden estimates suggest that nearly 800,000 individuals are permanently disabled or die annually due to diagnostic errors in the United States alone. The "Big Three" disease categories—vascular events, infections, and cancers—account for over half of these serious harms.
Research by Singh et al. (2013) found that cognitive factors, such as the failure to consider the correct diagnosis, and system factors, such as inadequate follow up of test results, are the primary contributors to these errors. Longitudinal health records directly address these failure modes by:
- Ensuring Continuity: Making prior results and clinical notes visible at the point of care.
- Supporting Reasoning: Providing the trending context that allows a clinician to spot patterns that a single data point would hide.
- Closing the Loop: Automating the tracking of abnormal results to ensure they are not lost to follow up.
Strategic Implementation for the Future
The World Health Assembly and the WHO Global Strategy on Digital Health endorse electronic health records as critical infrastructure. They are the only way to improve the quality, accuracy, and timeliness of information when it matters most.
For healthcare founders and institutional leaders, the strategy is clear. Investing in platforms that prioritize longitudinal data tracking is the most effective way to improve clinical outcomes. By making the patient history organized, visual, and accessible, we bridge the gap between fragmented data and diagnostic excellence.
Final Thought
We often look to the future for medical breakthroughs, but the most effective way to improve healthcare today is to better utilize the data we already possess. The patient story is the most important data point in medicine. Ensuring this story is preserved, tracked, and accessible is not just a technological upgrade; it is a clinical imperative that saves lives.
Fresh Perspectives, Timeless Wisdom Explore Our Latest Blog Edition
View All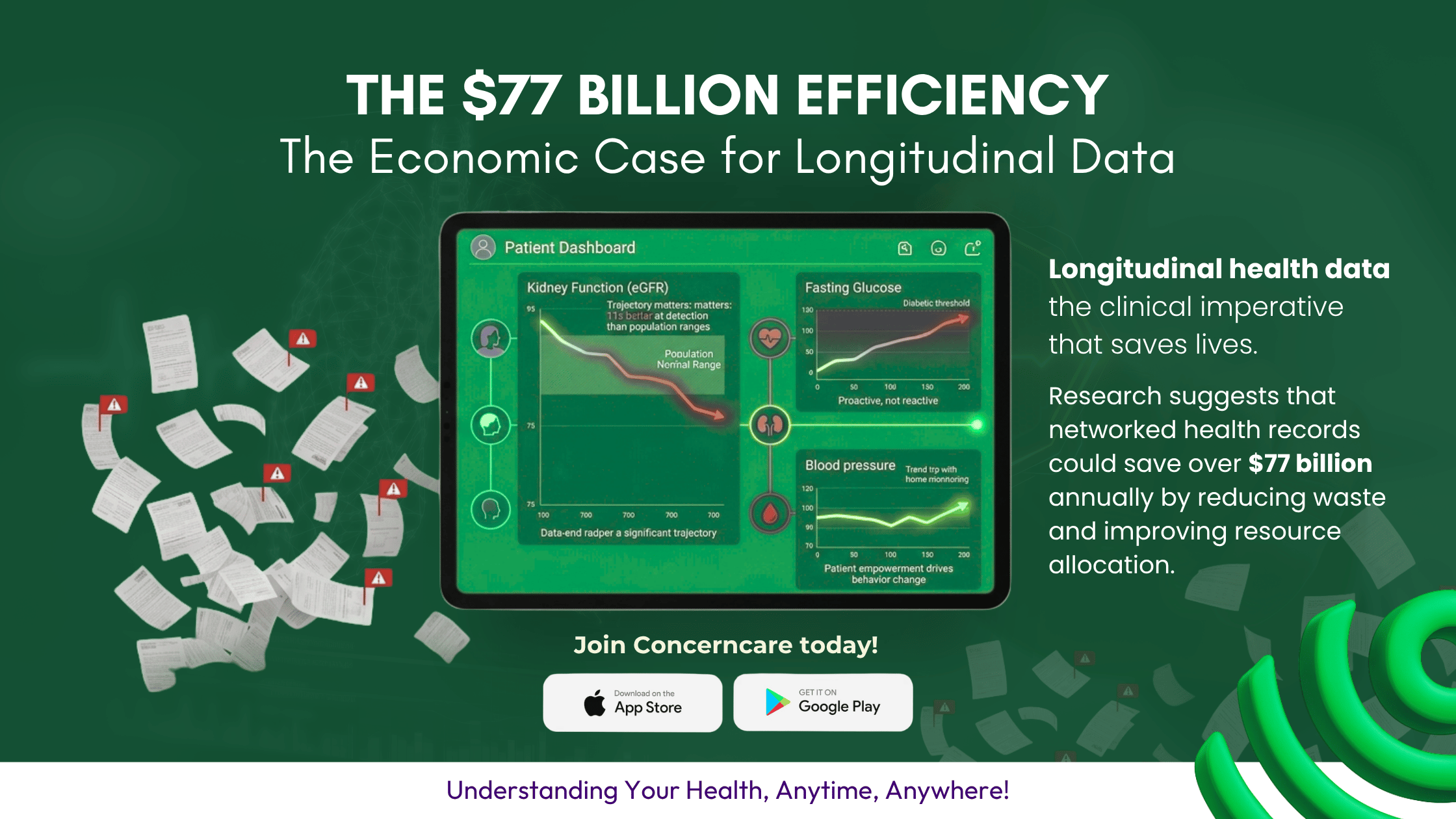
Join our newsletter to stay up to date on features and releases
Stay in the loop with exclusive updates, sneak peeks, and insider tips that will elevate your experience. Don’t miss out